
A manual for ending war and disease using financial incentives, pragmatic trials, and the radical assumption that humans respond to money. Spoiler: they do. 10.7 billion lives at stake.
Using data to minimize human suffering and optimize life for everyone. A better world through math.
A manual for ending war and disease using financial incentives, pragmatic trials, and the radical assumption that humans respond to money. Spoiler: they do. 10.7 billion lives at stake.

What if we took 1% of global military spending ($27.2B/year) and used it to actually save lives? 10.7 billion deaths averted. The maths checks out. The species does not.

The FDA's efficacy testing kills 3,070 people for every 1 it saves. 102 million dead since 1962. That's 17 Holocausts, but with better paperwork.

6,650 diseases have zero FDA-approved treatments. Pragmatic trials cost $929 vs $41,000. Scale them up and you get $0.84 per DALY. That's cheaper than a Mars bar. Why haven't we done this?

The US spends 3% more of GDP on government than Switzerland yet lives 6.5 fewer years. What if we just... looked at what works elsewhere and did that? Causal inference says yes.

Voter preferences have near-zero effect on policy. Citizens want 45:1 medical research vs military spending, but get the reverse. RAPPA fixes this with a slider and a dream.

What if saving millions of lives was a good investment? IABs pay 272% ROI to investors who bribe politicians into doing their jobs. Global household wealth is $454T. Opposition is $5T. Do the maths.

Civilization runs at 51.9% efficiency. The governance gap costs $101 trillion/year—$50,500 per household. We're leaving $1.16M per person on the table because meetings run long.
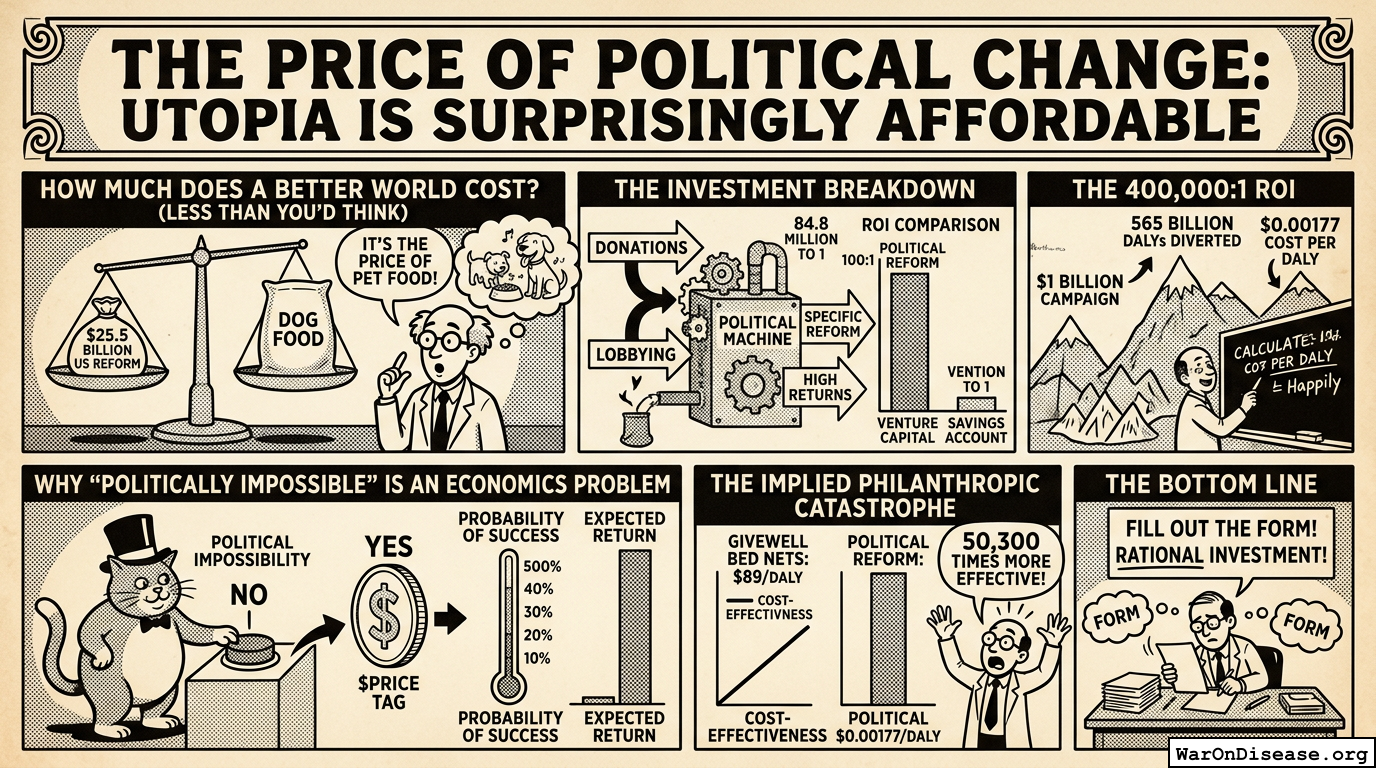
The maximum cost to reform all US policy is $25.5 billion. The return is $84.8 quadrillion. That's an 84.8 million:1 ROI. The real question isn't can we afford it, but why haven't we bought it.

Pragmatic clinical trials: current $0.5B, optimal $50B (9,900% underinvestment). Military: current $850B, optimal $459B. Agricultural subsidies: optimal $0. This spreadsheet is devastating.