A Tale of Two Trials
The difference between efficient and inefficient trial design isn't theoretical. Your species accidentally ran a controlled experiment on itself during COVID. Two countries. Same disease. One spent like it was trying to cure death. The other actually did.
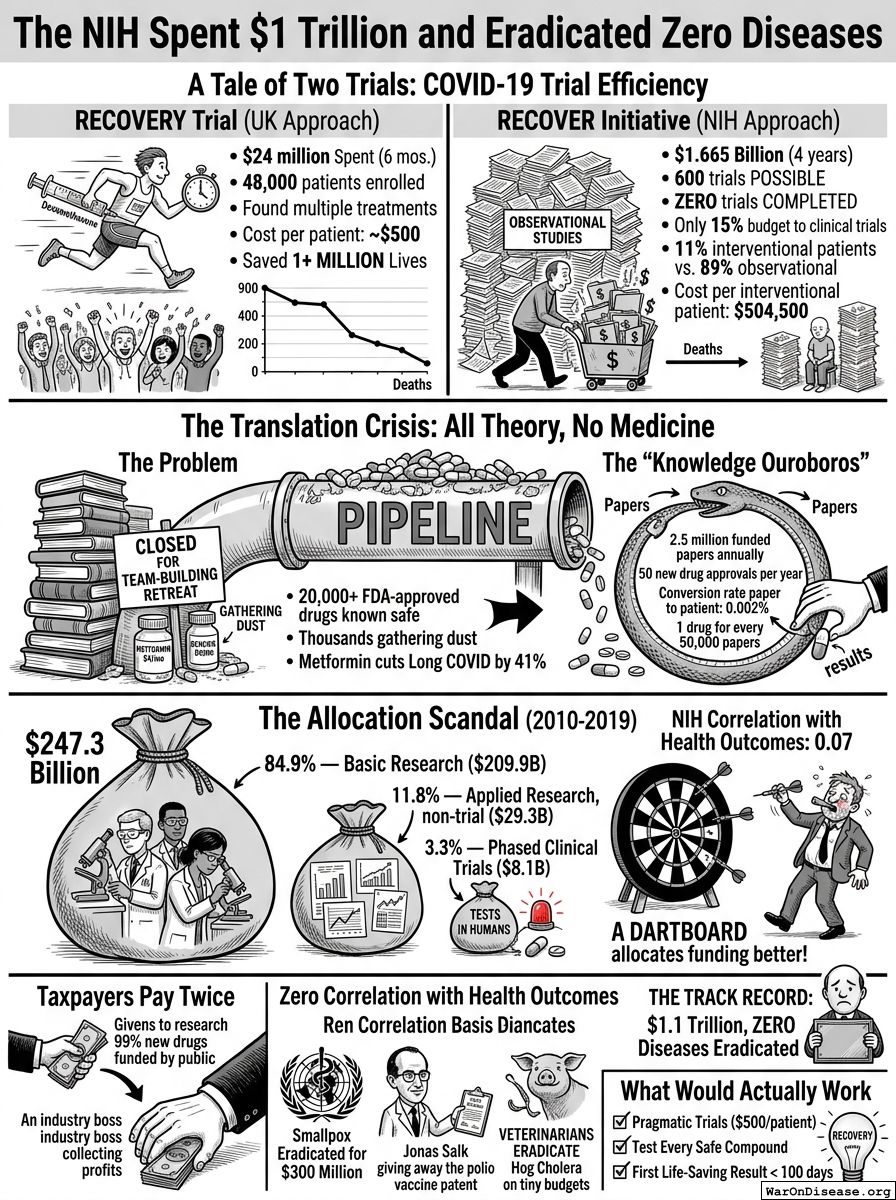
RECOVERY Trial (UK Approach)
The British spent $24 million over 6 months. Enrolled 48,000 patients. Found multiple effective treatments, including dexamethasone—a steroid that had been available since 1957. It reduced COVID deaths by one-third and saved over one million lives. Cost per patient: ~$500.
RECOVER Initiative (NIH Approach)
Nearly 600 potential treatments for Long COVID have been identified. At RECOVERY trial efficiency ($500/patient, 5,500 patients per treatment), $1.665 billion buys 600 completed trials. The NIH received $1.665 billion. Over 4 years, they completed zero.
Only 15% of the budget went to clinical trials; the rest funded observational studies, data management, and administration. Of those enrolled, roughly 11% were in interventional trials that actually tested treatments. The other 89% were in observational studies, which is the medical equivalent of taking attendance at a funeral.
Cost per interventional patient: $504,500, the price of a house. Nobody got a house and nobody got cured. They got observed. Expensively. The observation was very thorough. It has been peer-reviewed. The peers also observed the patients. The patients are still sick, but they are the most well-documented sick people in the history of sickness.
Six hundred trials were possible with that money. Zero were completed. That is the difference between a system that tests treatments and a system that tests patience.
The Translation Crisis: All Theory, No Medicine
Basic research is not the problem. Five decades of NIH-funded science built one of the largest drug candidate pipelines in history. The problem is what happens after the discoveries are made: almost nothing. The pipeline is full. The exit is closed.
There are over 20,000 FDA-approved drugs that are known to be safe in humans. Thousands more clinically-tested candidates are gathering dust, including over 3,000 marketed drugs that could be repurposed for diseases nobody's tried them on. You have a warehouse of safe molecules that have never been systematically tested for new uses. The warehouse is full. The testing facility is closed for a team-building retreat.
Then there's metformin. A phase 3 randomized controlled trial showed it reduces long COVID incidence by 41%. It costs $4 a month. It has been generic for decades. The NIH guideline response: "insufficient evidence to recommend for or against." Long COVID costs $170 billion a year. The $4 pill that cuts it by 41% has no corporate sponsor, because nobody profits from a generic. This is the entire chapter in one sentence.
The NIH is, by its own metrics, a publishing house that occasionally dabbles in medicine. It publishes 2.5 million funded papers annually. It produces approximately 50 new drug approvals per year. That's a conversion rate from paper to patient of 0.002%. For every 50,000 papers, one drug reaches a human. The rest become citations in other papers, which become citations in other papers, in an infinite loop of academics reading each other's homework. On Wishonia, we call this a "knowledge ouroboros." It looks productive from the inside. From the outside, it's a snake eating its own tail and writing a paper about the nutritional content.
The Allocation Scandal
Your National Institutes of Health has the word "Health" in its name and an annual budget of $47 billion. 47.5 million of you die annually from disease. You would think those two facts would be related. They are not.
Of $247 billion the NIH spent over a decade, exactly 3.3% went to testing which of the thousands of known-safe treatments actually work in humans. The other 96.7% funded understanding disease mechanisms, translating discoveries toward (but never into) clinical use, training scientists, and observational programs that spend billions watching disease without treating it.
3.3% on trials might be defensible if the testing queue were empty. It isn't. There are roughly 20,000+ compounds with established safety profiles, and 99.999997% of their possible disease applications have never been tested. Most are off-patent, which means no pharmaceutical company will fund trials for them, which means the NIH is the only entity that could, which means it is specifically choosing not to do the one thing only it can do.
It's like spending 96.7% of your grocery budget on cookbooks and 3.3% on food, then wondering why you're starving. Except the cookbooks are very prestigious and the starving people aren't on the committee that decides whether to buy more cookbooks.
The Receipts: Where $247.3 Billion Went (2010-2019)
- 84.9% — Basic research ($209.9B): Understanding disease mechanisms, molecular biology, genomics. Essential for identifying new targets, but 85 cents of every dollar is a lot of understanding and not much testing.
- 11.8% — Applied research, non-trial ($29.3B): Translating discoveries toward practical use, but without the final step of testing them in patients.
- 3.3% — Phased clinical trials ($8.1B): The only category that directly tests whether treatments work in humans.
Why This Allocation Exists
This is not the fault of individual researchers. Most became scientists because they wanted to cure diseases. The system they work in rewards everything except curing diseases.
Huge drug companies with political influence love the NIH. Taxpayers absorb the risk of basic research; industry patents whatever works. It's like if your neighbor paid for your kitchen renovation, and then you charged them rent to eat there.
But independent trials comparing drugs head-to-head? Those are terrifying. They might reveal that the $80,000 drug works about as well as the $4 generic. When Congress created PCORI (the Patient-Centered Outcomes Research Institute) in 2010, industry successfully lobbied to prohibit it from making coverage recommendations based on cost-effectiveness. Congress literally passed a law saying "don't fund research that might lower drug prices." They wrote it down. In legislation. On purpose. With their names on it. And then they went home and told their constituents they were fighting for affordable healthcare, because your species' capacity for doublethink is genuinely Olympian.
The 3.3% allocation isn't a mystery. It's a business model. Basic research produces publications. Publications produce tenure. Tenure produces more grants. Actual treatments are a byproduct that occasionally happens when someone forgets to optimize for papers and accidentally optimizes for results instead. It's like a restaurant where the chefs are passionate about food but get promoted based on how many menus they print. The menus are exquisite. They have won awards. The diners are eating the menus. Nobody has mentioned this.
You Pay Twice
Taxpayers funded research behind 99% of new drugs (356 drugs, 2010-2019). Industry patents the winners. The public pays again through high drug prices. When research leads to a dead end, the public eats the loss. You pay for the lottery ticket. They cash the winnings. You'd think someone would have mentioned this arrangement before now, and someone has, many times, but the people who cash the winnings also fund the campaigns of the people who could change the arrangement, so the arrangement continues.
The Patient Disconnect: Zero Correlation with Health Outcomes
Correlation between NIH funding priorities and actual disease burden: 0.07.
That is not a typo. On a scale of 0 (random) to 1 (perfect), the NIH scores "basically a coin flip." A dartboard would allocate research funding more rationally. A drunk person throwing darts at a list of diseases would produce a funding allocation that correlates more closely with actual disease burden than the National Institutes of Health, which employs 20,000 people and has been doing this for 50 years. The dartboard doesn't even need to be in the building.
The Track Record
$1.1 trillion over 50 years. Zero diseases eradicated. I asked the NIH how many diseases they've eradicated. They sent me a 40-page document about their strategic vision. I read all 40 pages. The number wasn't in it. The word "eradicate" wasn't in it either. The word "strategic" was in it 31 times.
The WHO eradicated smallpox for $300 million. Jonas Salk developed the polio vaccine in a university lab and gave it away for free, which is why nobody at the NIH talks about him at parties because he makes everyone look bad by comparison. He gave away the patent. I asked an NIH official what would happen if they gave away patents today and they made a sound I can only describe as a laugh, but sadder.
Veterinarians have eradicated multiple animal diseases on budgets the NIH would consider a rounding error. Your veterinarians eradicated hog cholera. Pigs. I should note the irony of humanity's failure to eradicate human diseases while more aggressively finding cures for animals you lock in metal crates too small to turn around in.
What Would Actually Work
The RECOVERY trial already proved it. $500 per patient instead of $50,000. First life-saving result in under 100 days. Over a million lives saved. The blueprint exists. It is not theoretical. It happened. In England. During a pandemic. While Americans were arguing about horse dewormer.
The British did not use a special technique. They did not have access to secret technology. They used the same drugs, the same disease, the same species of patient. They just tested the drugs on the patients instead of writing about the drugs near the patients. This is the breakthrough. It took zero breakthroughs.
Now imagine the other timeline. If the NIH had allocated even 20% of its $1.1 trillion to pragmatic trials over 50 years (the remaining 80% still on basic research), that produces 440 million patient-trials at RECOVERY efficiency. That is enough to test every safe compound against every major disease, multiple times, with replication.
The difference between that timeline and this one is not a matter of hindsight. Pragmatic trials existed the entire time. The efficiency data was available for decades. You chose the other road. It led here. I am told that on your planet, describing this situation accurately is considered "rude." On Wishonia, not describing it would be considered "complicity." I will risk the rudeness.
Comments