What If Drug Testing Was Cheap, Fast, and Not Completely Insane?
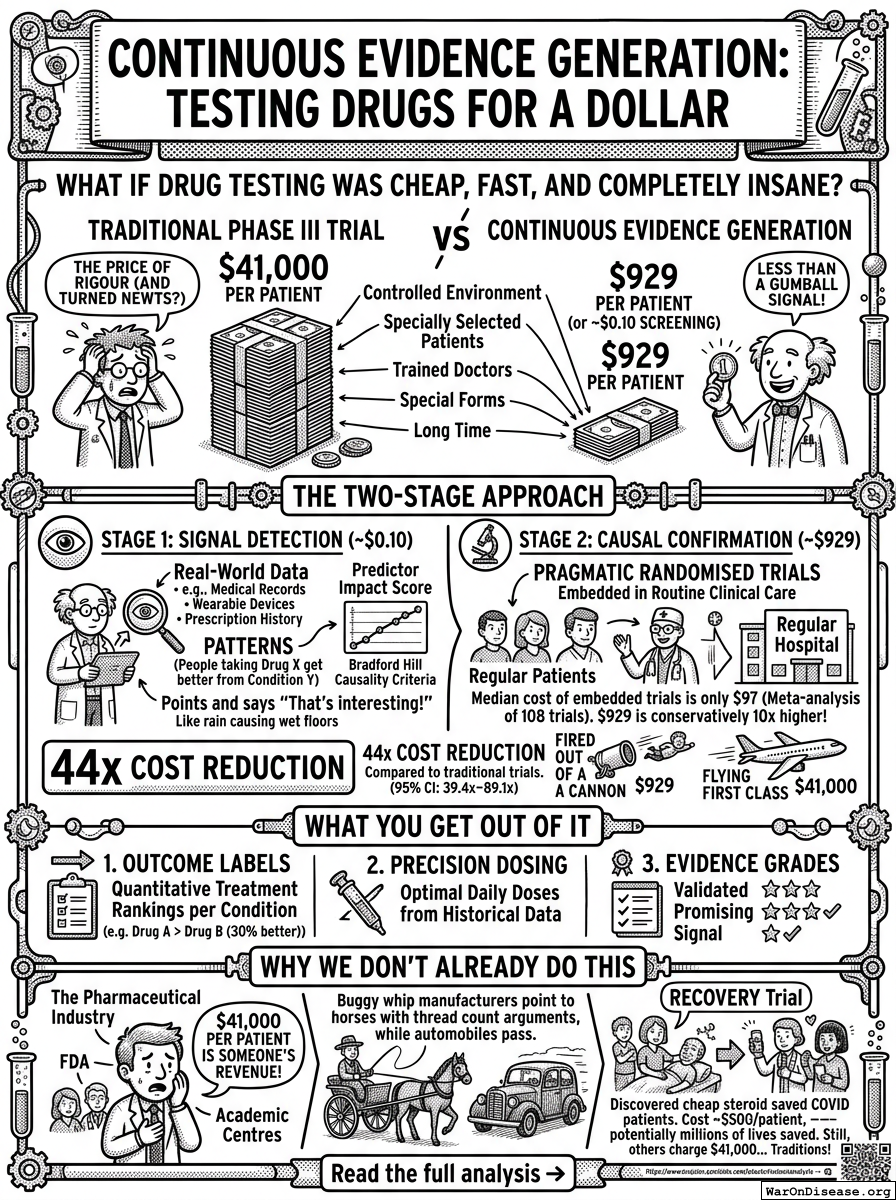
Currently, testing whether a drug works costs about $41,000 per patient in a Phase III clinical trial. This is the price of science, we're told. The price of rigour. The price of making sure your medicine won't turn you into a newt. Forty-one thousand dollars per person, in a controlled environment, with specially selected patients, monitored by specially trained doctors, filling out specially designed forms, for a specially long time.
The Continuous Evidence Generation Protocol proposes doing the same thing for $929 per patient. Or, in the initial screening stage, for approximately 10 cents.
Ten cents. That's less than a gumball. For a dime, you can find out whether a drug shows any signal of working. The fact that we've been spending $41,000 per person to do this is the kind of institutional insanity that would be hilarious if it weren't, you know, killing millions of people.
The Two-Stage Approach (Or: Why You Should Check Before You Commit)
Stage 1: Signal Detection — Cost: ~$0.10 per patient
This stage takes real-world data that already exists—medical records, prescription histories, wearable device data—and looks for patterns. "People who take Drug X seem to get better from Condition Y." It doesn't prove anything. It just points and says "that's interesting, someone should check."
This is analogous to noticing that every time it rains, the floor is wet. You haven't proven that rain causes wet floors—maybe someone's spilling tea. But it's a reasonable signal worth investigating, and it cost you nothing because you were going to look at the floor anyway.
The method uses something called a Predictor Impact Score, which quantifies the Bradford Hill causality criteria, which is a scientific way of asking "does this really cause that, or is it just a coincidence?" Bradford Hill was an epidemiologist who in 1965 laid out the rules for determining causation, and we've been largely ignoring them in favour of spending $41,000 per patient ever since.
Stage 2: Causal Confirmation — Cost: ~$929 per patient
Once Stage 1 identifies a promising signal, Stage 2 confirms it using pragmatic randomised trials embedded in routine clinical care. "Embedded in routine clinical care" means the trial happens inside regular hospitals with regular patients, rather than in a specially built facility with specially recruited participants who don't represent anyone except themselves.
A meta-analysis of 108 embedded pragmatic trials found a median cost of only $97 per patient. The $929 figure is deliberately conservative—about 10 times higher than the median—because the researchers apparently felt guilty about how cheap this was and rounded up to seem more respectable.
The 44x Cost Reduction
Combining both stages, the protocol achieves a 44.1x cost reduction (95% CI: 39.4x–89.1x) compared to traditional trials. At the upper end of the confidence interval, it's an 89x reduction. This is not a marginal improvement. This is the difference between flying first class and being fired out of a cannon—both get you there, but one costs considerably less.
What You Get Out of It
The protocol produces three types of outputs:
Outcome Labels: Instead of the current binary "FDA approved" or "not FDA approved," drugs get quantitative treatment rankings per condition. "Drug A works 30% better than Drug B for your specific situation" is more useful than "both are approved, good luck."
Precision Dosing: Optimal daily doses derived from historical outcome data, rather than the current system where the dose is whatever worked in the trial and you just have to hope you're similar to the trial participants. You probably aren't, because you weren't allowed in the trial.
Evidence Grades: A three-tier system—Validated, Promising, and Signal—combining both observational and experimental evidence. This is like a restaurant rating system, but for whether you'll survive.
Why We Don't Already Do This
The honest answer is: because $41,000 per patient is someone's revenue. The pharmaceutical industry has built itself around expensive trials. The FDA has built itself around reviewing expensive trials. Academic medical centres have built themselves around running expensive trials. Nobody whose salary depends on a $41,000 price tag is going to be thrilled about a $929 replacement.
It's the same reason buggy whip manufacturers were unenthusiastic about the automobile, except in this case the buggy whip costs $41,000 and the horse is dying while the manufacturers argue about thread count.
The RECOVERY trial in the UK—which cost about $500 per patient and discovered that a cheap steroid saved COVID patients—demonstrated that this approach works in practice, not just in theory. It potentially saved over a million lives. The rest of the medical establishment responded by continuing to charge $41,000 per patient, because traditions are important.
Comments