The Most Cost-Effective Medical Intervention in History
The Oxford RECOVERY trial isn't theory. It's proof.
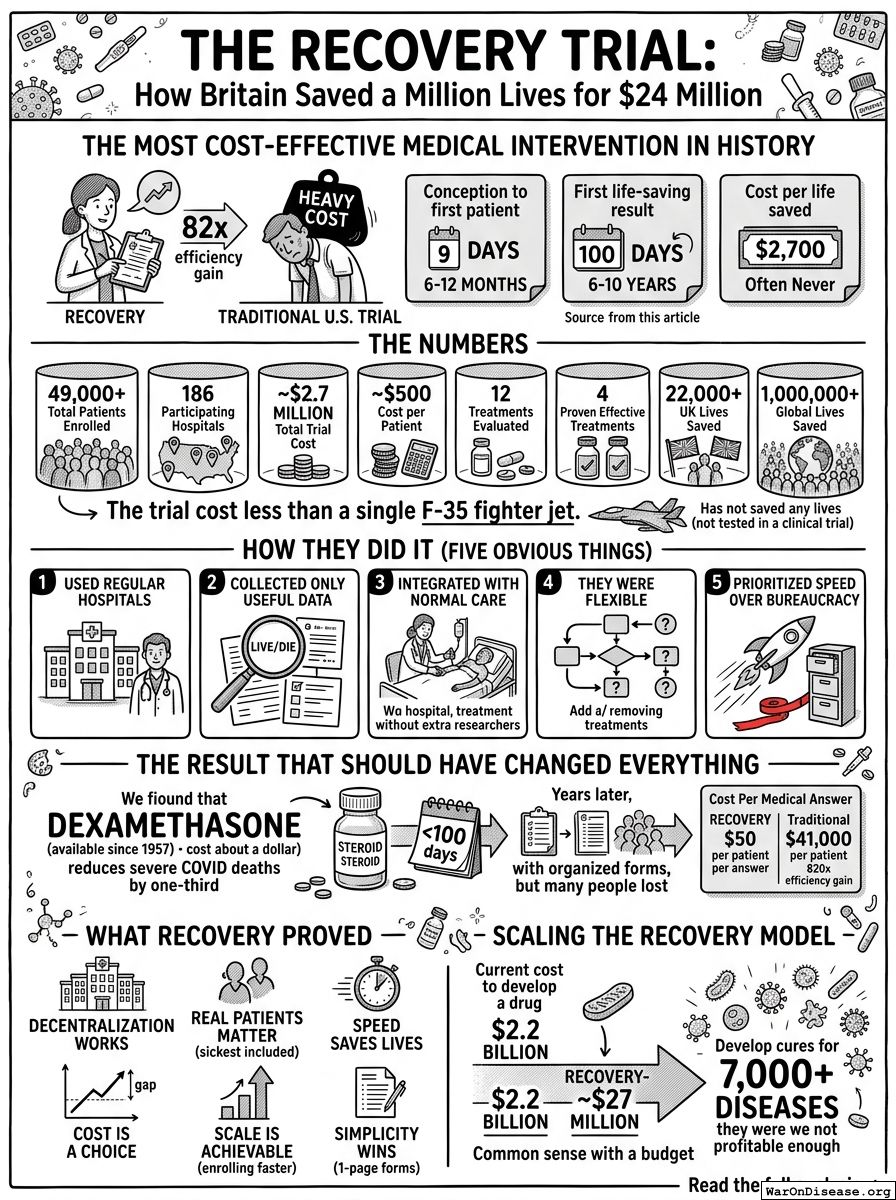
In 2020, Oxford spent $500 per patient. Traditional trials cost $41,000. RECOVERY saved over 1 million lives. That's an 82x efficiency gain. Achieved by doing five obvious things in obvious ways.
| Metric | RECOVERY | U.S. Average |
|---|---|---|
| Conception to first patient | 9 days | 6-12 months |
| First life-saving result | 100 days | 6-10 years |
| Cost per life saved | $2,700 | Often never saves any lives |
Let that last row sink in. The British spent $2,700 per life saved. The American system spends $41,000 per patient and frequently saves nobody, because by the time the paperwork is done, the disease has moved on to killing the next generation.
The Numbers
| Metric | Value |
|---|---|
| Total Patients Enrolled | 49,000+ |
| Participating Hospitals | 186 |
| Total Trial Cost | ~$2.7 million |
| Cost per Patient | ~$500 |
| Treatments Evaluated | 12 |
| Proven Effective Treatments | 4 |
| UK Lives Saved (by March 2021) | 22,000+ |
| Global Lives Saved (by March 2021) | 1,000,000+ |
| Days to First Major Result | <100 |
The RECOVERY trial enrolled 49,000 patients across 186 hospitals, tested 12 treatments, saved a million lives, and cost less than a single F-35 fighter jet. The F-35 has not saved any lives, though to be fair, it hasn't been tested in a clinical trial. Nobody would fund one.
How They Did It (Five Obvious Things)
1. They Used Regular Hospitals
No specialized research centers. No gold-plated equipment. Just regular hospitals with regular doctors treating regular patients. The same doctors who were already there, doing the same doctoring they were already doing, except now some patients got the experimental drug and someone wrote down what happened. Revolutionary.
2. They Collected Only Useful Data
The trial focused on core outcomes: "Did the patient live or die? Did they get better or worse?"
No seventeen-page questionnaires about quality of life. No daily blood draws for biomarkers nobody understands. Just: "Did it work?"
They used existing hospital data. One standardized form. Done. The entire data collection process for one of the most important clinical trials in medical history fits on a form shorter than what you fill out to join a gym.
3. They Integrated With Normal Care
Patients got the experimental treatment during regular care. No separate facility. No hovering clipboard researchers. Just normal doctors, except some patients got the experimental drug. Turns out this works fine. Who knew.
4. They Were Flexible
When a treatment didn't work, they stopped testing it. When a new promising treatment emerged, they added it. The FDA would require a completely new trial for each change. RECOVERY just... changed. Like adults making decisions in real time about things that matter. A concept so radical it apparently needed to be invented by the British during a pandemic.
5. They Prioritized Speed Over Bureaucracy
RECOVERY wanted to know if the drug worked and wanted to know fast. The FDA wanted to know if you filled out the forms correctly. These are different priorities. One of them saves lives. The other one has a filing cabinet.
The Result That Should Have Changed Everything
$500 per patient vs the U.S. average of $41,000 per patient. That's an 82x efficiency gain achieved by doing the obvious things in obvious ways.
Also, they saved a million lives by determining that dexamethasone—a steroid that has been available since 1957—reduces severe COVID deaths by one-third. Within 100 days. The cure had been sitting on a shelf for 63 years. It cost about a dollar. Nobody thought to test it because nobody makes money from a dollar drug, and nobody funds trials for drugs that cost a dollar, because the business model of clinical research requires the drug to be expensive enough to pay for the clinical research.
A trial following traditional timelines would likely still be in its early phases. The million people saved would be dead. The steroid would still be on the shelf. The forms would be very well organized.
Cost Per Medical Answer
- RECOVERY: $50 per patient per answer (12 treatments, 49,000 patients)
- Traditional U.S. trials: $41,000 per patient, usually testing one treatment
- 820x efficiency gain per medical answer
$41,000 to answer a question the traditional way. $50 to answer it the RECOVERY way. You could answer 820 questions for the price of one. You answer one.
What RECOVERY Proved
Six things that should be tattooed on the foreheads of every FDA bureaucrat:
- Decentralization works. 186 hospitals. Better results than centralized control.
- Real patients matter. Traditional U.S. trials exclude the sickest people. RECOVERY included them. Turns out testing drugs on the people who are actually dying produces more useful data about whether the drugs stop people from dying. This should not have been a revelation.
- Speed saves lives. 100 days to first result. Traditional: years.
- Cost is a choice. The 82x gap is bureaucracy, not capability.
- Scale is achievable. 49,000 patients enrolled faster than most U.S. trials enroll 1,000.
- Simplicity wins. Three 1-page forms vs. FDA's multi-form protocols.
Scaling the RECOVERY Model
Apply RECOVERY's approach to all drug development:
- Current cost to develop a drug: $2.2 billion
- RECOVERY-style cost: ~$27 million
- Efficiency gain: 82x
That's not a rounding error. That's an entirely different universe of possibility. At $2.2 billion per drug, only diseases that affect enough rich people get cures. At $27 million per drug, you can test treatments for everything. Including the 7,000+ diseases that currently have zero approved treatments, because nobody thought they were profitable enough to bother.
You know how to do this 82x more efficiently. Oxford proved it. During a pandemic. While the world was falling apart. The question isn't whether this works. The question is whether you'll scale it or keep spending $41,000 per patient while people die waiting in a queue that's been growing since 1962.
The British didn't discover a new technique. They discovered that not wasting money is cheaper than wasting money. Sometimes the breakthrough is just common sense with a budget.
Comments